Tooth Extraction Oral Surgery
The most common myth that exists among patients is, “My wisdom teeth came in and moved my teeth, making them crowded in the front, so I want to remove them so it doesn’t get worse.” HUGE MYTH. It is almost impossible for that to happen. The upper teeth and lower teeth occlude or come together in harmony. So, if your wisdom teeth came in and cause all your bottom teeth to move forward then your teeth would come together appropriately and you would not be able to close your mouth! The real reason a patient should extract their wisdom teeth is if they are impacted, and can cause harm to the nerve if not extracted in time. Also, if there is a huge food trap causing recurring infections, decay in both the wisdom tooth and the tooth in front of the wisdom tooth, which can cause both teeth to go bad. Furthermore, it is extremely difficult to keep the area all the way in the back of the mouth clean. Usually, even after brushing appropriately and flossing, there always remains a lot of plaque and or food stuck in the back of the mouth.
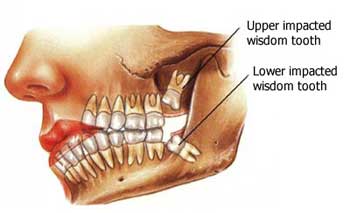
The infection of a tooth and the gums is called Pericornitis. It is caused by a bacterial overgrowth in the area of the wisdom tooth from bacteria that lives in plaque and calculus, which occurs because the area is very hard to keep clean. This is usually due to partially impacted teeth. Teeth become impacted when they are prevented from growing into their normal position in the mouth by gum tissue, bone, or other teeth. Impact is a common reason for the extraction of wisdom teeth. Extraction is the best method of treatment to prevent further problems. Another treatment is removing the gums in that area, which is done by a laser in our office. Teeth may also be extracted to make more room in the mouth prior to straightening the remaining teeth (orthodontic treatment), or because they are so badly positioned that straightening is impossible. Extraction may be used to remove teeth that are so badly decayed or broken that they cannot be restored. In addition, patients sometimes choose extraction as a less expensive alternative to filling or placing a crown on a severely decayed tooth. This is usually a last resort and is not recommended since teeth do not grow back.
In some situations, tooth extractions may need to be postponed temporarily. These situations include:
- Infection that has progressed from the tooth into the bone. Infections may make anesthesia difficult. They can be treated with antibiotics before the tooth is extracted.
- The patient’s use of drugs that thin the blood (anticoagulants). These medications include warfarin (Coumadin) and aspirin. The patient should stop using these medications for three days prior to extraction and always requires a clearance to do so by the patients being treated by a medical doctor.
- Patients who have had any of the following procedures in the previous six months: heart valve replacement, open heart surgery, prosthetic joint replacement, or placement of a medical shunt. These patients may be given antibiotics to reduce the risk of bacterial infection.
How do we remove teeth?
We do not actually “pull” teeth. Actually, we “push” or elevate teeth. The patient is always numb and feels virtually nothing. We would never complete a procedure such as an extraction unless the patient is numb. We do not want to cause any pain or harm. Tooth extraction can be performed with local anesthesia if the tooth is exposed and appears to be easily removable in one piece. An instrument called an elevator is used to loosen (luxate) the tooth, widen the space in the bone, and break the tiny elastic fibers that attach the tooth to the bone. Once the tooth is dislocated from the bone, it can be lifted and removed with forceps. After the extraction, depending on the case, some patients may require sutures. Depending on the case, one may have self-reabsorbing sutures, or silk sutures that need to be removed by the dentist.
Preparation
Before an extraction, the dentist will examine the patient’s medical history, noting allergies and prescription medications. A dental history is also taken, with particular attention to previous extractions and reactions to anesthetics. The dentist may then prescribe antibiotics or recommend stopping certain medications prior to the extraction. The tooth is placed under an X-ray to determine its full shape and position, especially if it is impacted.
If the patient is going to have deep anesthesia, he or she should wear loose clothing with sleeves that are easily rolled up to allow for an intravenous line. The patient should not eat or drink anything for at least six hours before the procedure. Arrangements should be made for a friend or relative to drive the patient home after the surgery.
Normal results
Depending on the case, if the tooth is removed simply, there may be LITTLE OR NO POST-OP pain or even swelling.
After an extraction, the wound usually closes in about two weeks. It takes three to six months for the bone and soft tissue to be restructured. Complications such as infection or dry socket may prolong the healing time.
What is a dry socket?

So, an extraction site has a blood clot at the side as a result of the extracted tooth. The blood clot is like a scab, except it does not fall off. It slowly turns into bone and gum tissue. If the blood clot falls out of the site, one may get what is called a dry socket. Any kind of action that will pull the clot out such as the vacuum effect of drinking from a straw, spitting hard, smoking, kissing, brushing the area hard, or any strenuous activity can cause the clot to fall out. If one is experiencing pain a few days after the extraction they may have a dry socket. Treatment of a dry socket includes numbing the patient, placing agitators to start bleeding again, or scraping the area to cause bleeding and make the blood clot form again.
Call (818) 751-5100